| Ally Anderson | Culture, civility, and psychological safety have been highlighted by recent national enquiries in maternity as being toxic and unsafe in units that have consistently failed women, their babies, and their families (Kirkup, 2015; 2022; Ockenden, 2022). Sound, evidence-based approaches to improvement that genuinely involve all staff groups and patients are needed to move forward and learn from these repeated mistakes and painful lessons (Dixon-Woods, 2022). A civil culture with good psychological safety for staff leading to improved patient safety is in line with South Tees Hospitals NHS Trust’s mission, vision, and values. In South Tees maternity, there was a recognition that the presence of psychological safety, which describes the ability to share ideas, concerns, or mistakes without fear of retribution (Edmondson, 2018) was at best, limited.
Methodology
A pilot session on psychological safety was held in December 2022, receiving overwhelmingly positive feedback. This was rolled out through ten further sessions between March-July 2023. All maternity staff were invited, participants across the full range of roles and grades attended. The sessions included reviewing what psychological safety is, discussions around culture, tools for feedback, and reviewing what maternity does well and what could be improved. Group work and polls from the sessions were collated and shared with the department leadership. | Building psychological safety into maternity services: an educational programme to support culture change.
 |
| Fransisca Retno Asih | Anemia during pregnancy is a major contributor to maternal deaths and poor births in both low- and high-income countries. On the other hand, hemoconcentrations, defined as hemoglobin values >130 g/L in the third trimester of pregnancy, have been linked to adverse effects on mothers and fetuses. These include preeclampsia and oxidative stress in mothers, as well as increased premature births, low birth weight, and a small gestation age for fetal pregnancy. The research aims to explore the low and high hemoglobin levels prevalence and characteristics among pregnant women. The design of this study is cross-sectional at the one of primary health care in Wongsorejo, Banyuwangi, Indonesia. Data was collected from October 2022 to October 2023. The data collected included age, gravidity, gestational age, and hemoglobin concentration. Institutional ethics approval was obtained from IThe Ethics Committee of the Institute of Health Science Banyuwangi. A total of 748 pregnant women were enrolled and analyzed by Chi-square test. 35.6% and 8.5% of pregnant women have anemia and hemoconcentration. 39.4% (295) of pregnant women come to have a hemoglobin check in the second trimester and only 24.5% (183) do in the first trimester. Anemia remains prevalent amongst pregnant women in Indonesia. Further studies and related evidence are needed on complaints that appear in pregnant mothers with high hemoglobin levels in the third trimester. Promotions aimed at raising public awareness to conduct the first contact antenatal care need to be enhanced. | Low and High Hemoglobin Levels Prevalence Among Pregnant Women in Indonesia.

|
| Martina Barbieri | In the paper it is discussed how midwifery’s sustainability stretches far beyond mere financial viability, in fact, its aim is to address the ethical perspective of the concept of sustainability in relation with midwifery care. Considering some key features of midwifery care, we tried to contextualize it in a Midwifery Care Ecosystem, of which we highlight three main aspects. Firstly, the relational sustainability of midwives, which is endorsed by the substantial role that relationships play in midwifery care and their implications for clinical and professional outcomes. Secondly, the relevance of the concept of ecology of care in midwifery is supported by its precise correspondence with the philosophical principles that underpin the profession, such as the respect for every personal expression of normality and the acceptance of diversities, which blur into cultural and social safety for women. The ecology of midwifery care, thus, highlights the sustainable and ethical aspects that support clinical practice. Finally, midwifery social sustainability lies in the implications midwives have, thanks to their practice. They serve as catalysts for community empowerment, advocates for health equity, and champions of social justice, shaping a more inclusive and resilient healthcare landscape. Within the Midwifery Care Ecosystem, stakeholders converge in a collaborative effort aimed at nurturing sustainable practices, heading toward ethical care delivery, embracing diversity, inclusiveness and respect. | Shaping Midwifery Sustainability: a discussion paper
 |
| Josephine Damus | Introduction and Aim:Nurses in Haiti, working in precarious conditions, have been classified at high risk of burnout. Knowing that midwives share the same conditions, we assessed the prevalence and determinants of burnout among them.Methods:This analytical cross-sectional study, including practicing midwives in Haiti, carried out from August to September 2023, used an online questionnaire collecting sociodemographic and professional factors as well as the Maslach Burnout Inventory, and performed chi-square test using Epi Info 7 software to test the associations.Results:Among 84 midwives, 100% were women, 55.95% aged 35 years or younger, 42.85% had at least ten years of experience. Considering the three dimensions constituting burnout, 72.62% of midwives had emotional exhaustion, 47.62% depersonalization, 54.76% a loss of personal accomplishment. The mean scores of the dimensions were 26.92, 5.13 and 37.69, respectively. The overall prevalence of burnout was 89.28%, divided into 25.00% severe (three dimensions affected), 35.71% moderate (two affected) and 28.57% low (only one affected). Working in a delivery room, a tertiary level facility, a private facility or more than 48 hours per week was associated with increased burnout prevalence, working in a family planning/sexually transmitted infection service, perceiving a fair distribution of work, or feeling safe was associated with decreased prevalence. | Prevalence and determinants of burnout among midwives in Haiti, August- September 2023
 |
| Sarah Esegbona-Adeigbe | This poster presents a research study on migrant Nigerian mother’s and midwives’ perceptions of cultural competency in antenatal care. Maternal mortality reports highlight that migrant Black women, particularly Nigerian women, have had up to a seven fold risk of dying in childbirth in the UK compared to other ethnic minority groups since 2000. Recent migration to the UK (less than five years), ethnicity and poor utilisation of antenatal care have been linked to maternal deaths. It is known that migrant African women are particularly vulnerable to poorer health in pregnancy related to poor pre conceptual care. Syndemic factors, which are defined as two or more diseases that synergise and worsen the burden of disease, as well as societal factors contribute to a woman’s risk of maternal mortality. In addition, there are complex causal pathways that are linked to maternal mortality and morbidity for Black women such as migration and socioeconomic factors. Cultural factors have been suggested as influencing Black women’s engagement with antenatal care yet there is sparse research in this area. | A Qualitative Study on Nigerian Mothers’ and Midwives’ Perceptions of Cultural Competency in Antenatal Care
 |
| Kristen Graham | The study identifies the challenges of midwives in providing quality emergency maternal and neonatal care under the themes of ‘Prepared’, ‘Willing’ and ‘Able’. The findings from surveys and interviews highlight the need to provide contextually appropriate education and training to prepare midwives to work in rural and remote work environments and to support midwives’ emergency care readiness through strengthened policy, health systems, supportive work environments and facility and referral capacities.In this poster, we present findings from a mixed-methods PhD study that explores the needs and opportunities for strengthening primary care midwives’ emergency maternal and neonatal care preparedness and readiness in rural and remote resource-limited settings. Study participants from sixteen countries include primary care midwives, midwifery educators, health service managers, ministry of health staff, and experts in midwifery and maternal and neonatal health. | Primary care midwives’ maternal & neonatal emergency preparedness & readiness in rural & remote resource-limited settings

|
| Christine East | Background: Postpartum blood loss volume has been commonly estimated through visual assessment, a method prone to intra- and inter-operator discrepancies, leading to concerns about underestimating blood loss. In 2019, Safer Care Victoria (Australia) introduced a Good Practice Point advocating the weighing/measuring of blood and related linen/items post-birth.Methods: This study retrospectively analysed maternity data collected at two co-governed Victorian maternity services (Hospitals A/B). It compared documented blood loss estimates, predominantly visually assessed, from 2016-2018, with those obtained 2020-2022 once weighing/measuring were promoted. An exploratory analysis categorized blood loss in 50mL increments (0-500mL) to consider the minimum reported volume at which weighing/measuring became more consistently implemented.Results: The adoption of weighing/measuring blood increased notably when reported volumes reached ≥350mL. By 2022, the rate of weighing/measuring with estimated blood loss (EBL) ≥350mL was 68% at Hospital A and 83% at Hospital B. Increased rates of reported blood loss ≥500mL were observed by the second epoch, particularly for 500 to MISSING TEXT | Exploring the Potential Link Between Routine Weighing/Measuring of Blood Loss After Vaginal Birth and Blood Loss Volume Assessment in Two Victorian Hospitals
 |
| Veronica Fernandez | Introduction: The postpartum period is critical to the physical and psychosocial health of the mother and newborn, including breastfeeding support and the transition to parenthood. Contemporary midwifery practice prioritizes maternal and child well-being while reducing environmental impact to ensure healthier future generations. Climate change poses a significant threat to global well-being, impacting vulnerable populations immediately and in the long term. Environmental factors during pregnancy affect postpartum mental health and can increase the risk of chronic diseases and complications. Sustainable midwifery practice aims to address these challenges holistically, benefiting both the individual and the environment.Objectives: This proposal aims to investigate the role of midwives in promoting sustainable environmental health through postpartum care and breastfeeding by focusing on community-based midwifery, environmentally-friendly reproductive health education, and integrating environmental approaches into midwifery practice.Methods: A review of the current literature on the role of midwives in environmentally friendly midwifery practice, specifically in postpartum care and breastfeeding, will be conducted using various online databases.Discussion: Community-based midwifery emphasizes holistic care during the postpartum period, addressing acute needs, maternal risks, and chronic conditions. Sustainable practices, such as judicious use of antibiotics and waste management, benefit both individual and environmental health. Breastfeeding promotion, aided by community support and education, is essential for infant nutrition and environmental sustainability. Challenges include environmental exposures that affect maternal and child health and barriers to breastfeeding, especially for working mothers.Conclusion: Community-based midwifery, which focuses on sustainable practices and environmental awareness, highlights the importance of holistic care and environmental stewardship for maternal and child health | Towards Eco-Friendly Midwifery: Nurturing Postpartum and Breastfeeding Care for a Healthy Future |
| Melanie Harington | Achievement of the United Nations (UN) Sustainable Development Goal (SDG) 3 (UN, 2015) by 2030 is in peril. This is illustrated by astronomical maternal mortality rates (UN, 2023), especially in sub-Saharan Africa (SSA). Universal access to modern contraception (MC) could half these deaths (United Nations Population Fund [UNFPA] et al, 2014) and midwives are uniquely placed to advance this effort (Nove et al., 2020). This poster will analyse the efficacy of the Accessible Continuum of Care and Essential Services Sustained (ACCESS) (Management Sciences for Health, [MSH], 2020) programme in Madagascar, which harnesses midwifery-led FP services, including MC, to reduce maternal mortality. ACCESS focuses on community development, whereby collective control remains within the hands of the community, which has been shown to be effective in a similar initiative in the Democratic Republic of Congo (Liebermann et al. 2019). The approach increases social capital (Baker, 1990), which Comfort et al., (2021) demonstrated increases likelihood of MC uptake. Thus, it is hoped that ACCESS will bring better health and higher MC uptake to local communities. Additionally, the programme addresses many barriers to MC in Madagascar such as travel distance, cultural barriers, and cost. (MSH, 2020; Ackerson & Zielinski, 2017).
The ACCESS programme is ongoing, so a formal evaluation is not yet underway, but the above analysis suggests that its methods are appropriate and initial feedback is promising. Should the formal evaluation confirm this assessment, the model could be replicated across SSA to reignite hope of achievement of SDG 3 by 2030. | Midwives Matter: Modern Contraception in Madagascar
 |
| Hanen Mrabet | Our project, showcasing the transformation of maternity triage at Al Wakra Hospital, embodies the VIDM 2024 theme, “Sustainable Midwifery: Caring for Tomorrow’s World,” by demonstrating a sustainable approach to improving maternal healthcare delivery. The initiative focused on enhancing the efficiency and effectiveness of obstetric care for patients with a gestational age ≥ 24 weeks, directly contributing to sustainable midwifery practices by prioritizing patient safety, minimizing wait times, and optimizing hospital resources.
Through the implementation of a robust triage system, guided by continuous SWOT analysis, PDSA cycles, and the integration of a dedicated, midwifery-trained triage team, we significantly improved patient flow and quality of care. This led to a drastic reduction in waiting times, from 31 to 14 minutes, and increased patient satisfaction to 97%. Such outcomes not only demonstrate immediate benefits but also highlight a sustainable model that can adapt to increasing demands and changing healthcare landscapes.
Our project illustrates how strategic changes in maternity triage can have a profound impact on maternal and newborn health, ensuring that resources are allocated
efficiently and that the care provided today supports the well-being of future generations. This initiative aligns with the global call for sustainable healthcare solutions by demonstrating how focused improvements in midwifery care can lead to lasting benefits for patients, healthcare providers, and the wider community. | Maternity Triage Patient Flow Optimization, Quality of Care Improvement.

|
| Lauren Papalia | Caesarean section birth (CS) accounts for 38% of Australian births and is known to negatively impact breastfeeding exclusivity and duration. Comparison of breastfeeding outcomes between elective (ELUSCS) and non elective lower uterine segment caesarean section (NELUSCS) births is needed to inform clinical care. Secondary analysis was performed on data from Australian women who had birthed by CS within the previous 12 months and completed an anonymous online questionnaire. Women responded to items relating to CS birth type and feeding methods immediately post birth, during the hospital stay and in the first 2 weeks at home. Self-reported pain at those time points was rated using a scale of 0 – 10 with 0 indicating no pain and 10 indicating severe pain. Associations between CS birth type, pain scores and feeding methods were determined, and breastfeeding prevalence at the time of survey completion examined. Our sample consisted of 851 women at 5 +/- 3.5 months postpartum, of which 435 (51.1%) were primiparous and 362 (42%) had a NELUSCS birth. Infants born by NELUSCS were more likely to receive formula (37.1% vs 28.8% ELUSCS, p = 0.024) and less likely to be breastfed (78.6% vs 85.9% ELUSCS, p = 0.022) during the hospital stay. During the 2 weeks after discharge women who birthed by NELUSCS had higher mean pain scores (6.5 vs 4.6 ELUSCS, p < 0.001). Few women expressed and fed their milk in the weeks after discharge, with higher rates seen after NELUSCS (7.7% vs 3.5%, p = 0.017). | Comparing Breastfeeding Outcomes of Australian Women who Birth by Elective and Non Elective Caesarean Section
 |
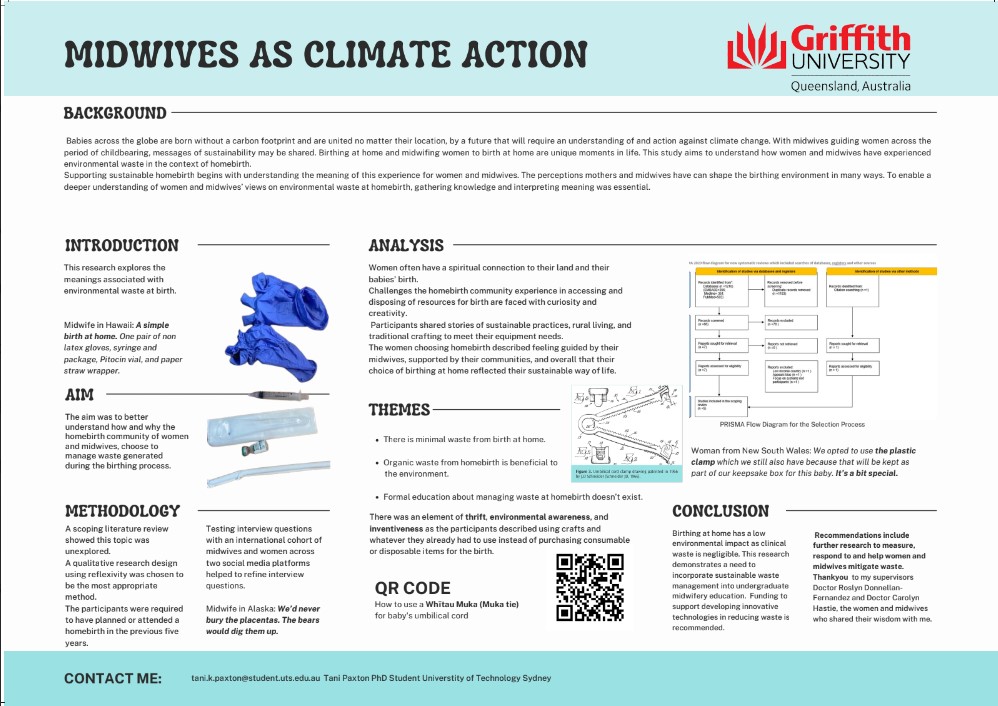
| Tani Paxton | This research explores the meanings associated with environmental waste at birth.The aim was to better understand how and why the homebirth community of women and midwives, choose to manage waste generated during the birthing process. There was an element of thrift, environmental awareness, and inventiveness as the participants described using crafts and whatever they already had to use instead of purchasing consumable or disposable items for the birth.This research demonstrates a need to incorporate sustainable waste management into undergraduate midwifery education. | Midwives as Climate Action
 https://vidm.org/wp-content/uploads/2024/04/Screenshot-2024-04-18-094232.jpeg https://vidm.org/wp-content/uploads/2024/04/Screenshot-2024-04-18-094232.jpeg |
| Vita Ratna Sari | Midwifery philosophy emphasizes woman-centered care, ensuring comprehensive services during pregnancy. However, implementing this philosophy in Indonesia requires advanced education and leadership skills. The International Confederation of Midwives Professional Framework provides a roadmap for improving midwives’ leadership skills, including clinical expertise, communication, professionalism, and advocacy. The Ruang Bidan Indonesia community organized a webinar to examine midwives’ leadership implementation and abilities in healthcare settings.
A mini leadership exercise was conducted with 25 participants in three focus groups, discussing the leadership role of midwives in healthcare systems. The group discussions were conducted online via Zoom Meeting, with facilitators leading each group. Participants were divided into three settings and participated in a rundown event.
The study highlights the diverse range of midwife-led care in Indonesia, highlighting both opportunities and challenges in various healthcare settings, particularly in hospitals and community health centers.
Furthermore, as a follow-up to focus group discussions from webinars and workshops on midwifery leadership that were held in 2023, Ruang Bidan Indonesia is hosting the Midwifery Leadership and Career Festival (MLCF) in honor of the International Day of Midwife (IDM) 2024, aiming to enhance midwives’ leadership skills and network with diverse mentors. | Empowering Midwifery: Navigating Challenges and Embracing Leadership for Woman-Centered Care in Indonesia

|
| Aqsha Wijaya | Midwives have a unique role in working with people and also a community to bring about cultural or behav¬ioural change that could have a direct impact on prac¬tice. Midwives are often con¬cerned with the experiences of people and how a diffi¬cult journey can be made more tolerable. It explained that a midwife needs to do research to improve their knowledge and their skills. Research plays a vital role in the practice of midwifery by informing evidence-based care, driving quality improvement efforts, advancing the profession, supporting informed decision making, addressing health disparities, and facilitating professional development. By doing research midwife will also learn how to be a research midwife or an academic midwife. A research midwife is usually works with team. Their area of practice includes the protection of human participants, care coordination and continuity, contributions to clinical science, clinical practice, and study management across a wide range of professional roles, practice locations, and clinical specialties. An academic midwife wil be the lead or co lead of the team who can decide several things. An academic midwife lead a research team for the entire research phase of the study, from conception to publication/dissemination, or they collaborate with the investigator team. Both of these professions provide excellent opportunity for midwifes to learn research skills while also participating in and leading research efforts. With a degree of knowledge, resilience, and determination, a midwife will be able to shape their research career and affect midwifery research in areas such as workforce, education, and practice. | A Research Career In Midwifery
 |
| Elizabeth Yip | Skin to skin and breastfeeding in theatre at birth and the effects on mothers and babies when it happens, or does not, has limited research. We need to understand the current reality to move forward. Breastfeeding success is caring for todays and tomorrow’s world.
Background: There is a limited body of evidence on the impact of caesarean section rates on a woman’s ability to experience some level of skin-to-skin contact with her newborn and establish breastfeeding.
Aim: To identify the incidence of skin-to-skin contact and breastfeeding in the operating space and explore the enablers and barriers to supporting this.
Method: A clinical audit consisting of 15 questions was developed. A staff survey, asking opened ended questions, was also administered. 365 audit forms were completed. Forty-one clinicians completed the survey.
Results: Just over 82% of newborns were held in the theatre (91% of these experienced some form of skin-to-skin). The major reason for limiting skin-to-skin contact was temperate of the theatre. 22% of newborns were reported to have breastfeed and /or attempted a breastfeed in theatres. Reported barriers to breastfeeding included: ‘awkward’ maternal positioning, maternal and/or newborn ill health after birth, workload and time pressures, insufficient education and support for staff and parents.
Discussion: This research offers valuable insights into real-world practices and staff attitudes, contrasting with idealised scenarios often found in published literature. Midwives and institutions can use this information for their professional development and support women. | Skin to skin and breastfeeding in theatre: Staff Survey  |
| Elizabeth Yip | Skin to skin and breastfeeding in theatre at birth and the effects on mothers and babies when it happens, or does not, has limited research. We need to understand the current reality to move forward. Breastfeeding success is caring for todays and tomorrow’s world.Background: There is a limited body of evidence on the impact of caesarean section rates on a woman’s ability to experience some level of skin-to-skin contact with her newborn and establish breastfeeding.Aim: To identify the incidence of skin-to-skin contact and breastfeeding in the operating space and explore the enablers and barriers to supporting this.Method: A clinical audit consisting of 15 questions was developed. A staff survey, asking opened ended questions, was also administered. 365 audit forms were completed. Forty-one clinicians completed the survey.Results: Just over 82% of newborns were held in the theatre (91% of these experienced some form of skin-to-skin). The major reason for limiting skin-to-skin contact was temperate of the theatre. 22% of newborns were reported to have breastfeed and /or attempted a breastfeed in theatres. Reported barriers to breastfeeding included: ‘awkward’ maternal positioning, maternal and/or newborn ill health after birth, workload and time pressures, insufficient education and support for staff and parents.Discussion: This research offers valuable insights into real-world practices and staff attitudes, contrasting with idealised scenarios often found in published literature. Midwives and institutions can use this information for their professional development and support women. | Skin to skin and breastfeeding in theatre: Clinical Audit  |
| Elizabeth Yip | A retrospective audit of medical records collected at a IBCLC run outpatients’ clinic (approved by NSLHD LEC 2021/ETH01012). Notes were screened and records included for women who had ongoing breast pain and who also had microbiology completed for areola swabs and/or milk (n=369), performed mostly by EY, in the preceding 8 years. Samples were collected on 440 visits: breast-swabs (715); milk samples (190).Reported pain started: first-week postpartum (263), week 2-5 (99); > 6 weeks (41). The length of pain ranged from < 1 week (39) to > 6 weeks. Over 50 different descriptions of pain were noted. Many reported at least 2 descriptive terms: predominantly painful (172), burning and/or stinging (125); sore (105); tender (28); unbearable (22). Of those recorded, treatments which stopped the pain/ helped the pain; range of antibiotics: (84/2); antifungals (28/4); kenacomb (26/6); bactroban (4/0). Microbiology of swabs (692): no growth (6); skin flora or gram + organisms (294); CNS (91); other bacteria (342). Most common bacteria were: penicillin resistant S.aureus (PRSA), penicillin susceptible S.aureus (PSSA), multiresistant S.aureus (MRSA) and Group B Streptococcus (GBS) with 1 to 3 different bacterial species commonly present. Candida species were seen in 8 samples. Of those women who had follow-up recorded; weaned (too painful) (26) mixed feeding (75) continued feeding (228) at next follow-up. Persistent breast pain in lactation is multifactorial and while blanket treatment with antifungals or antibiotics is not appropriate in all cases, it is in some. This study highlights the need for microbiota assessment so that appropriate personalised treatment can be delivered. Although it does not give answers to the conflicting advice, it adds to the limited information available for women with ongoing breast and nipple pain. As seen by the data this is very relevant to all who care for women and babies. | Pathology of nipple and areola in lactating women with ongoing pain – Which microorganisms play a role? (A retrospective analysis of previous clinical care) |










 https://vidm.org/wp-content/uploads/2024/04/Screenshot-2024-04-18-094232.jpeg
https://vidm.org/wp-content/uploads/2024/04/Screenshot-2024-04-18-094232.jpeg





{kind=link}